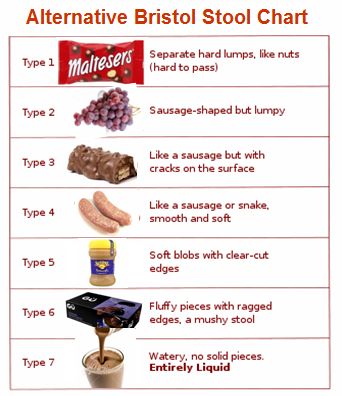
Alternative Bristol stool form chart from rewarm.co.uk
.
On Thursday 1st August at 8pm, the #PooPride tweet chat with We Nurses took place – woo  hoo!
hoo!
.
.
Having been on twitter for a little over a year, I’ve seen lots of topics discussed. Bowel problems aren’t one of them. Which is odd, given the effect many psychiatric medications have on your digestive system. My hints on twitter about my debilitating bowel problems seemed to go unnoticed. However, since there are a lot of people taking psychiatric medications, and for long periods, there must be a lot of people out there with constipation and other bowel problems who are suffering in silence.
At Easter, Charlotte Walker (@BipolarBlogger) blogged about a weekend away and how medication and bowel problems had affected her. I recognised the juggling act and stress of taking medications and planning toilet breaks. Then, yesterday evening, I spotted a tweet by Charlotte about constipation, to which I responded. When Charlotte asked me if I had any recommendations, it turned out that, after years of managing my own bowel problems, I could come up with 20 off the top of my head! (See below.)
That started up a spontaneous tweet chat. (All the tweets are linked below.) Then, because the issue is much wider than our personal experiences, because people were suggesting medications and treatments to try, and because constipation can cause serious complications, I decided to see if we could have an organised tweet chat involving medical professionals too. Watch this space!
Here’s the tweet of Charlotte’s that caught my eye:
“Dear antipsychotics, love what you’re doing on the bipolar, great stuff. Just concerned my bowel may RUPTURE, ease off a bit there, maybe?”
Charlotte explained that she was experiencing antipsychotic-induced chronic constipation which had flared up into faecal impaction. Not fun. Not fun at all.
Problems with your digestive system – whether it’s too much movement, or too little, or both; whether it’s frequency, consistency or volume; or colour, smell, blood or mucus; or some other charming symptom – can be a blush-making topic. I know, because I’ve blushed those blushes.
The first time I plucked up courage to mention to a medical professional the bowel problems I was experiencing, I received a reaction I hadn’t anticipated: laughter. As a result, I didn’t raise the issue again till an Atos medical. Through bodily sobs and streaming tears caused by shame, I forced myself to describe my symptoms. This time, the reaction was disbelief: zero points. Laughter; then disbelief. After that, through trial and error, a keen memory for toilet locations and a well-stocked handbag, I gradually found ways to manage my bowel problems myself.
That was no longer possible, however, when I was detained in hospital. The combination of enforced inactivity, a diet devoid of fibre and the side effects of psychiatric medications meant my bowels came to a halt. There was one fortnight when I passed just one motion. Thank goodness for stretchy trousers that could accommodate my massive and growing belly, taut as a drum, as I waddled round the ward in pain, unheeded and untreated except for senna.
Since then, through my own efforts and working with my GP and the specialists she’s referred me to, I’ve found a way to manage the problems. And I can talk to pretty much any health professionals without embarrassment now so I know that, if problems come up in future, I’ll be able to talk about them and, hopefully, get the help I need.
You know you’ve got constipation when your digestive system has slowed down so you pass motions less often than you want to or when your stools are hard and difficult to pass. You may also have indigestion. It’s uncomfortable. It’s embarrassing. It’s even potentially dangerous. It’s an important topic.
Normally, constipation is a short-term problem which responds well to lifestyle changes and, if necessary, treatment. However, if constipation is drug-induced and there isn’t an alternative, you may be looking at a multi-pronged approach in order to successfully keep on top of constipation. So, for those of us taking medication, it’s a topic of even more importance.
Below, as a starting point for discussion, as food for thought, are the twenty tips I came up with off the top of my head for Charlotte to try out, plus a few more I thought of later. They are things that have helped me personally (or people I know) to manage the impact of drug-induced constipation. They’re aimed at someone who’s otherwise physically healthy. They’re tips you could use as a springboard for discussion. They’re common sense, not rocket science. They’re not comprehensive. For medical advice, take a look at the NHS website or ask your medical practitioner. Maybe they’re worth a try. We’re all different, after all.
As Charlotte tweeted later that evening:
“Goodness! What a lot of people have followed me since @Sectioned_ and I started talking about constipation! #goodtoshare”
And, as Phil Dore (@thus_spake_z) tweeted:
“Poo Pride! :D”
.

My personal tips on dealing with drug-induced constipation:
1. Keep a poo diary
If you keep a record of the motions you pass, you may start to see a (monthly or other) pattern. Women in particular can find their bowel movements are affected by their monthly cycle. Maybe it’s not a relapse or a remission; it’s just your monthly cycle. If you get to know the effect (if any) that your monthly cycle has on your bowels, you’ll be better able to distinguish what works and what doesn’t for your constipation. And improving constipation involves trial and error.
What to include in the poo diary? Time of day you pass (each) motion, what you were doing at the time (eg had you just smoked a cigarette). You’ll need to keep a record of what you eat and and your fluid intake, to see what effect that has too.
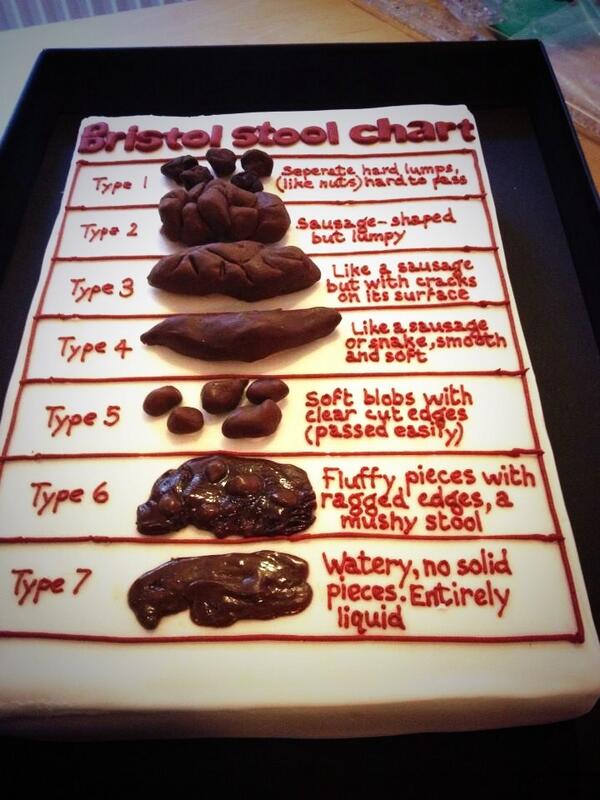
Also, include your Bristol stool scale number. It classifies stools into 7 different types. The ideal is around around a 3 or 4. The official Bristol stool form chart is above.
Bear in mind when looking at the chart above that your poo may not be the same as the colour shown: stools vary in colour depending on what you’ve eaten. I’ve pooed red after beetroot juice and green after spinach. Taking an iron supplement can (I’m told) blacken stools (and harden them). If there’s blood or mucus in your poo though, that’s not a good sign. Mention it to your medical practitioner.
Such a detailed diary won’t be necessary forever, but it’s a useful tool to see where you are now, and to identify any patterns emerging. Try to keep one for at least 2 weeks (men) or two cycles (women).
2.Eat or drink something
Stimulating one end of the alimentary canal (the long tube that runs from your mouth to your bum) can stimulate the other. Therefore, when you want to poop, first eat or drink something. I find that, if it’s going to work, it does so within around half an hour. So if I need to leave the house by 10am, I’ll eat drink or something (however light) at 9am to give it a chance to work its magic.
3. Try a stool softener
An effect of some psychiatric medications is to reduce the fluid content of foods. A stool softener (or osmotic laxative) is a medication that draws water into the stools, making them softer and therefore easier to pass. Lactulose is the stool softener I’ve tried and it’s worked for me. Brilliantly. Movicol is another one, though I haven’t tried that.
A downside is its taste: exceptionally sweet. But hey, just clean your teeth afterwards. Especially as another side effect of some psychiatric medications is dry mouth, or rather reduced saliva – and hence reduced protection for the teeth.
4. Use a jug
If your problem is hard stools, it’s water that will soften them; so you’ll need to take in sufficient fluids during the day. To ensure I push through enough fluids, I fill a jug with water on rising and fill my glass from it throughout the day. That gives me a goal to work through during the day.
Don’t drown yourself in fluids late in the day and end up wetting the bed. And yes, I have done this too: the meds I take knock me out so I sleep like the dead and wake up in a puddle. The way round that is to spread my fluid intake throughout the day so it’s not gulped down in a rush towards bedtime.
5. Prunes
Fluids rock. As do prunes. Drinking prune juice helps me too. And it’s super yummy. As are prunes with custard. I’ll take any excuse to eat prunes.
Beware though: don’t take too many. Once, before I knew the laxative effect of prune juice, I drank a whole litre in one go. That’s how I know it works. Now, I just drink a glass.
6. “Doing a Paula”
If you’re just not going, your bowels may be sluggish. Your digestive transit time (the time it takes from something going in your mouth to it coming out the other end) may have been slowed – whether caused by medications, or enforced inactivity if on ward, or lack of motivation to get active (a side effect of some drugs). If you want to know your transit time, you can do the sweetcorn test (eat some sweetcorn and see how long it takes to spot it in your stool – transit time should be around 24 hours).
One way to get the bowels moving is high impact exercise, which can stimulate the bowel to open. If I’m indoors, I’ll fire up my trampet and bounce along for a song. Jogging works too. Just be sure you know those toilet locations or have a handy pack of tissues in your bum bag.
Incidentally, if you normally have healthy bowels but find yourself almost or actually involuntarily evacuating your bowels during a run (pooing yourself), that may not necessarily mean you have a bowel problem. It can happen to normal, healthy runners the world over. It’s an occasional downside of the pastime. After all, the phrase “Doing a Paula” derives from the reason Olympic athlete Paula Radcliffe had to retire from the Athens marathon. Don’t panic. Just plan ahead. And learn the technique that enables you to delay passing a motion.
7. Vitamin C
Heard of the vitamin C “bowel tolerance dose”? Taking over 1g vit C gives me the trots. Everyone’s dose is different. I know the trots aren’t ideal, but sometimes you just need to pass a motion.
Incidentally, if you’ve recently changed your diet to include a high dose vitamin C supplement and find your stools are loose, the vitamin C could be the problem. Don’t automatically assume you’ve caught a bug or got IBS (irritable bowel syndrome). Experiment with the dose till you find the one that works for you.
8. A bathroom step
Essential bathroom kit is a little step (about 8” high), so that, when you sit to poo, your knees are a little above your bum. Sitting in this position relaxes your lower body and places your bowel in the correct position to pass a motion easily. It reduces the need to strain (which risks causing haemorrhoids/piles). And, bonus, it also means you can rest your reading material on a flat surface!
They’re cheap as chips (mine cost £2). Once you’ve used one of these, you’ll never want to poop any other way. If you’re visiting, you can usually find something to stick under your feet – eg a couple of thick books, a pack of loo rolls – so your knees are at the right height. Simples.
9. Try training/routine
This is a controversial point because some bowel specialists I’ve seen say it’s impossible to train the bowel and others say the opposite.
The idea is that, at the same time each day – eg half an hour after breakfast (when you’ve stimulated the bowel by drinking or eating something) – you go into the bathroom whether or not you want to pass a motion. A sort of potty training for adults. You sit on the toilet, hang out there for 5 minutes, then leave. If you pass a motion good; if not, no problem. Maybe next time.
10. Latex gloves
This comes from a little trick I recall my mother showed me as a child. To get newborn kittens to poop for the first few weeks, rub their little bottoms. It worked. Why wouldn’t it work for humans too?
The idea is to very gently circle the anus with a gloved finger to relax it and, hopefully, give it that little extra nudge it needs to stimulate the passing of a motion. Use lubrication of some sort (eg vaseline).
11. Smoking
Seriously. There’s a reason people smoke after a meal! I nearly took it up in hospital again because I was so blocked. (Also because only the smokers were allowed into the garden.) Before I became a non-smoker, smoking a cigarette was a guaranteed way to bring on what I believe the Girl Guides call the “daily clear out” (though I suspect they don’t get the little girls to smoke).
12. Coffee
Again, there’s a reason people drink coffee after a meal. If you don’t like the taste, think of it as medicine: it may not taste good but, if it does the job, that’s what matters.
13. Stimulant laxatives
Senna is a laxative that works by stimulating the muscles of the gut to push your poo towards the anus (a stimulant laxative). Maybe this is just what you need. Bear in mind though that that senna is aimed at relatively short term use because it can, over time, make your bowels lazy.
Personally, senna was not good for me. When the nurses offered me various medications on ward, I made the mistake of thinking that, because it is a natural product, it would be the best choice. Wrong.
In fact it’s what caused me to blow up like one of the sheep in Far From the Madding Crowd: I wanted someone to spike me in the guts to relieve me of the terrible pain. I felt like I was going to die. In one fortnight, I only passed one motion. I didn’t know what was causing the problem. I thought I’d be even worse without the senna. Luckily I was able to speak to a hospital pharmacist for an hour, and he helped me to work out what the problem was and what would help. If in doubt, seek medical advice.
Bulk-forming laxatives such as Fybogel are a third type, which help stools retain fluids.
14. Fibre
It’s a key recommendation for the prevention and management of constipation to have sufficient dietary fibre. Most adults don’t eat enough, and constipation is your clue that that means you. You can increase your fibre intake by eating more fruit, vegetables, wholegrain rice, wholewheat pasta, wholemeal bread, seeds, nuts and oats. Eating more fibre helps keep bowel movements regular by helping food pass through your digestive tract more easily. High fibre foods can also make you feel fuller for longer, in case you’re struggling with cravings (another side effect of psychiatric drugs which contributes towards weight gain).
If you decide to increase your fibre intake, however, do so gradually: a sudden increase may make you feel bloated, produce more flatulance and give you stomach cramps. Eek!
15. There may be no magic bullet
Bear in mind that, though the hard stools and slow transit may be caused by psychiatric drugs, they may not be fixed just with drugs. It may take a package of measures to bring constipation under control. But finding the right drug/combination can surely go a long way to helping.
And be prepared for the fact that you may end up taking more drugs to deal with side effects (like constipation) than the number of drugs you take for your primary psychiatric symptoms. That’s just the way it is. Just as every surgery causes scars, so every drug has side effects. It’s just a question of finding the side effects profile you’re prepared to live with.
16.Experiment
You could try each of these suggestions to see which ones work for you. Perhaps put them together into a morning routine, tweaking as you go to work out the right combination for you: we’re all different. However, it’s hard to tell what’s working when you’re doing lots of different things at the same time. You could consider doing them all at the same time and then gradually cutting each one out, one by one, to see what works; or stopping everything then adding them back in one by one.
17.Input and output
Reducing food intake (a little) can help. I wouldn’t have got quite so bunged up if I hadn’t eaten quite so much! Obviously we all vary and some people are under-weight or need to follow a special diet. On the whole, however, many of us would benefit from cutting down a little on what we eat. And, the less you put in, the less there is to get stuck inside!
18.Wet food
If the problem is constipation & hard stools, eating “wetter food” (eg soups, stews, curries) can also help a little. If you live on crisps, you’re asking for trouble.
19.We can all learn
Even clued up healthy eaters who think they know a lot about diet and lifestyle may benefit from a food diary & having their diet tweaked by a dietician. I’ve learned new stuff from the professionals I’ve seen. Even if we’re doing everything we know 100% spot on, science might have moved on since then. There are lots of fad diets and food myths we might have fallen prone to without noticing, so reviewing a food diary or having a professional do so can lead to improvements – even small tweaks – being found. And, with constipation, it’s these little things that add up.
We might even learn that things we thought were healthy options were actually contributing to bowel problems. For instance, taking supplements is always good, right? Wrong. For instance, taking too much vitamin C can cause loose stools, whilst taking iron tablets can harden stools. Fibre is always a good thing, right? Wrong. For some, a high fibre diet can irritate the bowel and lead to bloating and frequent loose stools. What you may think is IBS may resolve entirely on a lower fibre diet. Exercise is always good for you, right? Wrong. For some, high impact exercise can lead to involuntary bowel evacuations (“Doing a Paula”). If so, stick to gentler exercise. Or practice bowel control techniques.
20.Try it
Even if you’ve tried something before, it may be worthwhile trying it again. Bowels can be contrary beasties. “I’ve tried everything already” may mean you miss out on doing something that now works.
21. Tummy massage
Another way to stimulate the bowels to start moving is with tummy massage. Use the heel of your hand to make a big circle in a clockwise direction (the direction the bowels go in). Alternatively, lie on a hard surface face down and roll around. Or lie on your back with your legs in the air and cycle, to get the tummy muscles moving. All very elegant!
22. A hot bath
As Sylvia Plath wrote in her novel The Bell Jar, “There must be quite a few things a hot bath won’t cure, but I don’t know many of them.” A hot bath is another great way to get the bowels moving.
23.Specialist help
Ask your GP for a referral to a specialist clinic. If at first they say there isn’t one (my otherwise excellent GP did), do your research so you know the right terminology to use when asking for the service. For instance, I’ve had referals to a community dietician; a colposcopy clinic; a continence clinic; a bowel education group; a colonoscopy consultant; and a hospital consultant for anatomical investigations.
24. A tricky balance
Once you start taking steps to actively treat constipation, you might push your bowels the other way. Oh joy! Your bowels become as unpredictable as climate change. You might swing back and forth between the two before getting it right. Ho hum. You’ll get there. And in the meantime, be prepared.
25. The pitfalls of syndromes
If, along your constipation journey, someone mentions IBS, be careful how you use the diagnosis. With family and friends it may provide a label that helpfully enables you to side-step that awkward conversation about symptoms. However, if you’re going for medical treatment and you mention IBS, you’ll most likely see the doctor’s eyes glaze over. In essence, a syndrome is the medical profession’s way of saying they don’t know what’s wrong with you. It’s saying you’ve got a collection of symptoms they don’t know how to treat. It is a label that says to a medical professional, “Nothing you do will make the patient better. Next!” Use with care.
If you have any tips for easing constipation that you’d like to share, please feel free to comment below. Happy pooing!
.
.

- My Storify of tweets – Psychiatric medication and constipation
- My Storify of tweets – the original 20 tips to beat constipation
- My Storify of tweets – some thoughts on starting a tweet chat on constipation
- Charlotte Walker’s blog post – Five hundred miles: remission versus recovery
- NHS Choices – Constipation
- My blog – Hot baths and how I relax
- Resources page – Medication – including links to the Choice & Medication website (“Probably the world’s biggest, best & most comprehensive independent website for partients, carers & professionals about choice & mental health medication.”) and The eMC (“The electronic Medicines Compendium (eMC) contains up to date, easily accessible information about medicines licensed for use in the UK)
- The healthy eating website produced by United Biscuits, manufacturer of biscuits and snacks, including McVitie’s biscuits, Jaffa Cakes, Hula Hoops, McCoy’s, Skips and KP Nuts. Yup, they have a healthy eating website. I read it on the back of my crisp packet.
.
.
.
Tags: advice, doctors, medication, Mental health, NHS, nursing, psychiatric wards, smokers, smoking